

Abstract
Introduction:
Several prognostic models for overall survival (OS) in chronic lymphocytic leukemia (CLL) have been developed, but none were derived for patients (pts) with relapsed or refractory (R/R) CLL treated in the era of novel agents. We used a comprehensive approach to derive and validate a novel risk model for OS in 2,475 pts with R/R CLL who received therapy in randomized phase 3 trials evaluating ibrutinib (IBR), idelalisib (IDELA), and venetoclax (VEN) vs control arms, or the Mayo Clinic CLL Database (MCCD).
Methods:
In collaboration with Janssen, Gilead, Pharmacyclics, and Genentech/Roche, the analysis included 2,475 pts from 6 multicenter randomized phase 3 trials or the MCCD. Trials included were: IBR plus bendamustine-rituximab (BR) vs placebo plus BR (HELIOS: NCT01611090), IBR vs ofatumumab (RESONATE: NCT01578707), IDELA plus BR vs placebo plus BR (Study 115: NCT01569295); IDELA plus rituximab vs placebo plus rituximab (Study 116: NCT01539512); IDELA plus ofatumumab vs ofatumumab (Study 119: NCT01659021); VEN plus rituximab vs BR (MURANO: NCT02005471). All pts had R/R CLL and required treatment by iwCLL criteria.
The model-building dataset (n=969) included pts from HELIOS and RESONATE, and was randomly assigned to the IBR/chemoimmunotherapy (CIT) training dataset (n=727) and IBR/CIT internal-validation dataset(n=242). Three independent external validation datasets included IDELA/CIT (n=897), VEN/CIT (n=389), and MCCD (n=220).
We applied univariate and multivariate analyses (MVA) to 28 candidate clinical/laboratory and genetic prognostic factors to derive the risk model in the training dataset. The primary endpoint was OS. We assessed the need for separate models for targeted agents by interactions with treatment in univariate analyses. We proceeded to develop a single model for all pts with R/R CLL, as only one candidate factor (del(13q), interaction p value <0.1) demonstrated a marginal differential effect.
We evaluated cutoffs for dichotomized covariates and for definition of risk groups after the final factors were selected. We fit a Cox regression on the training and internal/external validation datasets using the risk categories as the covariate to test the difference among the groups, and calculated the C-statistic as a measure of discrimination.
Results:
Of 11 selected factors with a significant univariate effect on OS (p<0.1), 6 were independently prognostic in the MVA of OS (p<0.05): Baseline β2-microglobubulin (B2M), lactate dehydrogenase (LDH), hemoglobin (HGB), IGHV mutational status, number of prior therapies, and time from initiation of last therapy.
We excluded number of prior therapies from the model, reasoning that its optimal cutoff might change with advances in CLL therapies. IGHV did not remain significant (p=0.0592) in MVA of 5 remaining prognostic factors. Notably, del(17p) was not independently prognostic for OS.
The final risk model consisted of 4 prognostic factors: B2M ≥5 mg/L, LDH elevated, HGB <110 mg/L for women or <120 mg/L for men, and time from initiation of last therapy <24 months. Because hazard ratios for each factor were similar (range, 0.55-0.68) with overlapping confidence intervals, 1 point was assigned to each factor. The resulting score separated pts into low (score 0-1), intermediate (score 2-3), and high risk (score 4) groups.
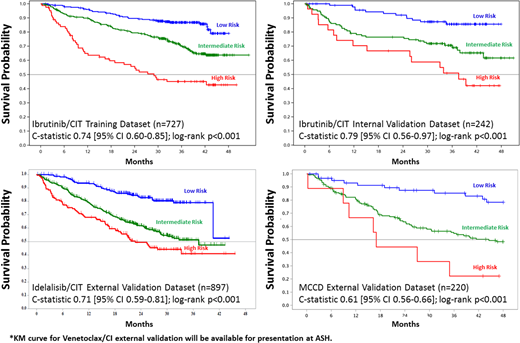
Our risk model was prognostic for OS in the IBR/CIT training dataset (C-statistic 0.74 [95% CI 0.60-0.85]; log-rank p<0.0001) and was validated in the IBR/CIT internal validation (C-statistic 0.79 [95% CI 0.56-0.97]; log-rank p<0.0001), as well as in all 3 external validations: IDELA/CIT dataset (CS=0.71, 95% CI 0.59-0.81; log-rank p<0.001); VEN/CIT dataset (CS=0.76, 95% CI 0.66-0.85; log-rank p=0.01); MCCD (CS=0.61, 95% CI 0.56-0.66; log-rank p<0.001).
Conclusions:
We present the first validated risk model for OS in R/R CLL in the era of targeted therapies. Our model consists of 4 readily available factors (B2M ≥5 mg/L, LDH elevated, HGB <110 mg/L for women or <120 mg/L for men, and time from initiation of last therapy <24 months), identifies 3 prognostic groups with significantly different OS, and has been validated for pts treated with all FDA approved targeted therapies: IBR, IDELA, and VEN. This identifies a well-defined cohort of pts with R/R disease with an unmet clinical need who are suitable for prospective trials targeting these pts. An exploratory analysis regarding prediction of MRD is ongoing.
Darif:Jannsen: Employment. Londhe:Jannsen: Employment. Xing:Gilead Sciences, Inc.: Employment. Mun:Genentech: Employment, Equity Ownership. Kay:Cytomx Therapeutics: Membership on an entity's Board of Directors or advisory committees; Pharmacyclics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Tolero Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Infinity Pharm: Membership on an entity's Board of Directors or advisory committees; Agios Pharm: Membership on an entity's Board of Directors or advisory committees; Morpho-sys: Membership on an entity's Board of Directors or advisory committees; Acerta: Research Funding; Gilead: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Shanafelt:Mayo Clinic: Patents & Royalties: Physician Well-being Index, Medical Student Well-being Index, Well-being index; GlaxoSmithKline: Research Funding; Genentech: Research Funding; Pharmacyclics: Research Funding; Janssen: Research Funding; Abbvie: Research Funding; Celgene: Research Funding. Furman:Loxo Oncology: Consultancy; Pharmacyclics LLC, an AbbVie Company: Consultancy; Sunesis: Consultancy; TG Therapeutics: Consultancy; Verastem: Consultancy; Gilead: Consultancy; Incyte: Consultancy, Other: DSMB; Acerta: Consultancy, Research Funding; Genentech: Consultancy; Janssen: Consultancy; AbbVie: Consultancy. Hillmen:Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Research Funding; Pharmacyclics: Research Funding; Alexion Pharmaceuticals, Inc: Consultancy, Honoraria; Novartis: Research Funding; Gilead Sciences, Inc.: Honoraria, Research Funding; F. Hoffmann-La Roche Ltd: Research Funding; Acerta: Membership on an entity's Board of Directors or advisory committees. Sharman:Acerta: Consultancy, Research Funding; Pharmacyclics, an AbbVie Company: Consultancy, Research Funding. Seymour:AbbVie: Consultancy, Honoraria, Research Funding; Celgene: Consultancy; F. Hoffmann-La Roche Ltd: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Genentech Inc: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Honoraria, Research Funding. Jones:Celgene: Employment, Equity Ownership. Ferrante:Jannsen: Employment. Dreiling:Gilead: Employment. Mobasher:F. Hoffmann-La Roche Ltd: Other: Ownership interests non-PLC; Genentech Inc: Employment. Stark:Genentech: Employment. Reddy:Actinium Pharmaceuticals: Employment, Equity Ownership; Pharmacyclics: Employment. Howes:Janssen: Employment. James:Pharmacyclics: Employment. Bhargava:Gilead: Employment. Zelenetz:Novartis/Sandoz: Consultancy; Abbvie: Research Funding; Celgene: Consultancy; Amgen: Consultancy; Gilead: Consultancy, Research Funding; AstraZeneca: Consultancy; Genentech/Roche: Consultancy, Research Funding.

